3D Facial Norms Technical Notes
- Overview
- Database Search
- Summary Statistics
- Tools
- Technical Notes
- Abstract
Overview
![]()
The 3D Facial Norms Database is a web-based resource designed to provide the research and clinical community with access to high-quality craniofacial anthropometric normative data. Unlike traditional craniofacial normative datasets that are limited to measures obtained with handheld calipers and tape measurers, the anthropometric data provided here are based on digital stereophotogrammetry, a method of 3D surface imaging ideally suited for capturing human facial surface morphology. Also unlike more traditional normative craniofacial resources, the 3D Facial Norms Database allows users to interact with data via an intuitive graphical interface and - given proper credentials - gain access to individual-level data, allowing users to perform their own analyses.
The content below is designed to give the user detailed background information on the 3D Facial Norms Database. It is critical that users understand the methods used to collect the data, to ensure proper interpretation and use.
If you require additional information, please contact the Principal Investigator, Seth M. Weinberg , PhD.
Kinds of Data Available
- 3D coordinates (x,y,z) for a variety of standard facial surface landmarks
- Selected linear distances calculated from 3D facial surface landmarks
- 3D facial surfaces in Object Wavefront (.obj) format
- Selected face and head measurements using traditional anthropometric methods (i.e., calipers)
- Basic demographic descriptors, such as age and sex
- Genotypic markers (coming soon)
Summary-Level vs. Individual-Level Data
3D Facial Norms data are available at both the summary level and individual level. This distinction has important implications for how users gain access to data.
Summary-level data include things like sex- and age-specific means and standard deviations for selected anthropometric measurements (e.g., the average intercanthal distance for five year old males). As such , all summary-level phenotypic data are non-controlled and available to all users directly on the www .facebase.org site.
Individual-level data refer to the unique data elements that comprise the summary-level data, and include things like the measurements, landmark coordinates and 3D facial surface files for each individual in the database. One major advantage with individual-level data is that the user can carry out their own statistical analyses on original raw data as if they collected the data themselves.
Access to all individual-level phenotypic data is controlled and only available to users with the proper permissions (see ).
In accordance with NIH policy, access to both individual-level and summary-level genotypic data is also currently controlled-access.
Potential Uses for the Data
Normative Control Data for Craniofacial Comparisons
Collecting craniofacial control data for comparison purposes is essential for many research questions about facial morphology. This can be a time consuming and expensive effort, and very often the resulting control samples are too small to fully capture the range of human facial variation. As a source of normative control data, the 3D Facial Norms Database is designed to facilitate the comparison of facial morphology at both the group level (e.g., comparing a new set of cases against 3D Norms controls) and the individual level (e.g., comparing a single patient or subject against a set of matched controls). Because the user can specify variables such as age, sex and ancestry, comparisons that require strict matching are possible. Further, morphological comparisons can be based on traditional linear distances, 3D landmark coordinates and/or entire 3D facial surfaces, allowing users to employ a wide variety of morphometric analysis methods.
Analyses of Human Craniofacial Variation and Growth Patterns
The large 3D Facial Norms Database is an excellent resource for exploring questions relating to patterns of human facial variation and growth; e.g., how does the face change over different life stages, how are sex differences manifested in facial structure, how are different facial structures integrated during growth, and what are the major facial differences among different ethnic/ancestral groups? These questions are of particular interest to those working within the fields of physical anthropology, orthodontics and forensics. In this context, 3D Facial Norms data can also serve as an out-group for comparison , be used to supplement or expand existing datasets, or serve as a replication dataset to validate prior results.
Genomic Studies of Quantitative and Qualitative Craniofacial Traits
One of the principal goals of the 3D Facial Norms Database is to provide researchers with the raw materials to explore the genetic basis of normal human facial variation. To this end, we expect in the near future to be able to make genome-wide SNP markers available along side our phenotypic data . Importantly, these data can also serve as an extension and/or replication arm for existing or planned GWA analyses of human facial traits.
Test-Bed for Developing Novel Image Analysis Methods
The thousands of 3D facial surfaces available through the 3D Facial Norms Database provide a unique resource for computer science and computer vision experts to develop novel surface-based methods for representing and analyzing human faces.
Process for Accessing Data
All summary-level phenotypic data are immediately available to all users through the main 3D Facial Norms project interface on the www.facebase.org site.
All individual-level phenotypic data and all genomic data are currently controlled-access. The process for obtaining permission to access controlled human data on FaceBase projects can be found on our Docs site .
In brief, the process involves the following steps:
- The user obtains appropriate ethics (IRB) approval at their institution.
- The user submits a Data Access Request (DAR) form and associated documentation to the FaceBase Data Access Committee (DAC) for review.
- Upon approval, FaceBase grants the user permission to access and download the requested data through the FaceBase.org site.
Data Use Restrictions
All users are encouraged to familiarize themselves with the FaceBase Data Use Certification (DUC) document, which covers all aspects of appropriate use for human data residing on the FaceBase site and the consequences for violating these policies.
Subject Recruitment and Demographics
In the current phase of recruitment, the 3D Facial Norms Database is targeting 3500 unrelated male and female individuals of European-Caucasian ancestry between the ages of 3-40 years, with (ideally ) a roughly equal number of persons in each age and sex category. The age categories breakdown as follows :
| Age Category | Ages (years, months) | Age Category | Ages (years, months) |
|---|---|---|---|
| 3 | 3y,0m - 3y,5m | 19 | 19y,0m - 19y,11m |
| 3.5 | 3y,6m - 3y,11m | 20 | 20y,0m - 20y,11m |
| 4 | 4y,0m - 4y,5m | 21 | 21y,0m - 21y,11m |
| 4.5 | 3y,6m - 3y,11m | 22 | 22y,0m - 22y,11m |
| 5 | 5y,0m - 5y,11m | 23 | 23y,0m - 23y,11m |
| 6 | 6y,0m - 6y,11m | 24 | 24y,0m - 24y,11m |
| 7 | 7y,0m - 7y,11m | 25 | 25y,0m - 25y,11m |
| 8 | 8y,0m - 8y,11m | 26 | 26y,0m - 26y,11m |
| 9 | 9y,0m - 9y,11m | 27 | 27y,0m - 27y,11m |
| 10 | 10y,0m - 10y,11m | 28 | 28y,0m - 28y,11m |
| 11 | 11y,0m - 11y,11m | 29 | 29y,0m - 29y,11m |
| 12 | 12y,0m - 12y,11m | 30 | 30y,0m - 30y,11m |
| 13 | 13y,0m - 13y,11m | 31-32 | 31y,0m - 32y,11m |
| 14 | 14y,0m - 14y,11m | 33-34 | 33y,0m - 34y,11m |
| 15 | 15y,0m - 15y,11m | 35-36 | 55y,0m - 36y,11m |
| 16 | 16y,0m - 16y,11m | 37-38 | 37y,0m - 38y,11m |
| 17 | 17y,0m - 17y,11m | 39-40 | 39y,0m - 40y,11m |
| 18 | 18y,0m - 18y,11m |
Because there are 35 age categories, this works out to 100 individuals per age group (50 males and 50 females) under an ideal recruitment scenario. The final recruitment numbers may ultimately vary from this ideal picture, but we are striving for no less than 30 individuals in any age/sex group.
The 3D Facial Norms Database is cross-sectional in design, so each individual is represented only once in the database.
The participants comprising the 3D Facial Norms Database were recruited at three main sites within the US:
- University of Pittsburgh, Pittsburgh, PA (under the direction of Drs. Seth M. Weinberg and Mary L . Marazita)
- Seattle Children's Hospital, Seattle, WA (under the direction of Drs. Carrie L. Heike and Michael L. Cunningham)
- University of Texas Health Science Center at Houston, Houston, TX (under the direction of Dr. Jacqueline T. Hecht)
Recruitment strategies vary from site to site but include the use of public print advertisements, word-of-mouth, direct mailing, university and hospital-based research registries, kiosks in public venues , and collaborations with general dental and medical clinics.
Screening Procedure
All participants are screened via interview to determine whether they meet our inclusion criteria :
- European Caucasian ancestry*
- Age between 3-40 years
*In addition to self-reported ancestry, subjects are asked to report the national origin of their maternal and paternal grandparents. All four grandparents must be of European origin.
All subjects are also screened on the following exclusion criteria:
- The presence of conspicuous facial hair
- The presence of any facial piercings other than small studs?
- A personal history of facial trauma or disfigurement?
- A personal history of facial reconstructive or plastic surgery?
- A personal history of orthognathic/jaw surgery or jaw advancement?
- A personal history of any facial prosthetics or implants?
- A personal history of any palsy, stroke or neurological condition affecting the face?
- A personal or family history of any facial anomaly or birth defect?
- A personal or family history of any syndrome or congenital condition with a facial manifestation ?
An affirmative response to one or more of the above items would disqualify an individual from participation in the study.
The Informed Consent Process
At each recruitment site, informed consent is obtained from all subjects by trained study coordinators prior to any data or sample collection. For minors under the age of 18, a parent or court-appointed legal guardian must be present and sign the consent document. Children who are old enough also co-sign an assent form. During the informed consent procedure, all subjects are told how their data will be shared and are given the opportunity to ask questions about aspects of the study.
The Study Workflow
Following informed consent, all subjects undergo a brief demographic interview. Subjects are then asked to provide a saliva sample using Oragene collection kits. A handful of measurements (described in detail elsewhere) are then obtained directly on the subject's head with the aid of spreading calipers . The subject's facial surface is then captured via 3D stereophotogrammetry.
The entire study protocol takes an average of 20 minutes.
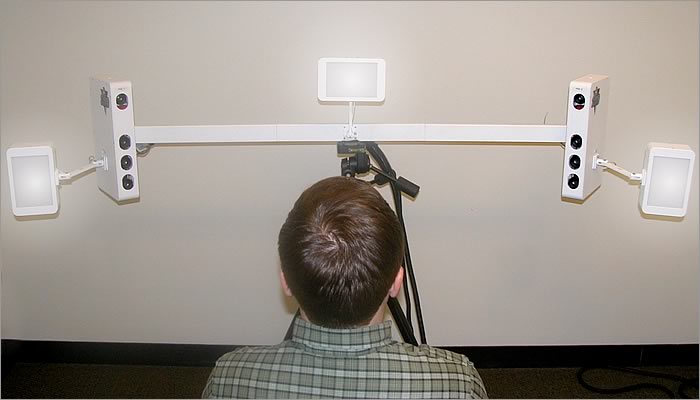
3D Facial Imaging Technology
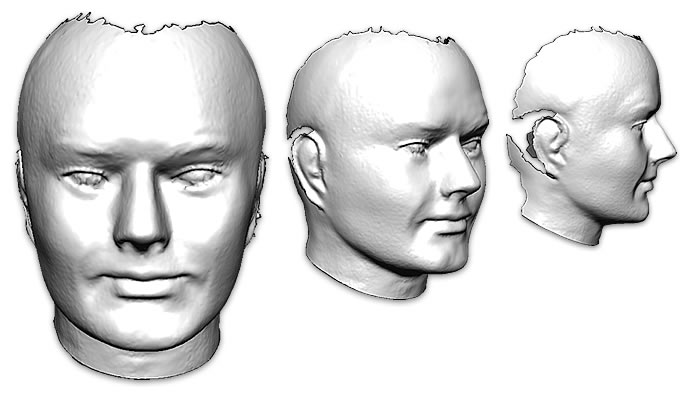
3dMD digital stereophotogrammetry imaging systems (Atlanta, GA; www .3dmd.com ) were used capture the facial surfaces of all subjects in the 3D Facial Norms Database . These systems are outfitted with multiple machine vision CCD cameras mounted at fixed angles and distances , to capture overlapping views of the face and head (the degree of coverage depends on the number of cameras). The entire capture process occurs in less than 2 milliseconds and results in the creation of a dense 3D point-cloud that conforms to the geometry of the face. For visualization purposes, the point-cloud can be connected to produce a 3D mesh and color/texture information can be mapped onto the underlying geometry allowing for photorealistic rendering. For those interested in a more technical description, please see Lane and Harrell (2008) .
Technical Validation Studies
A number of independent investigators have assessed 3dMD systems in terms of measurement accuracy and precision. In a recent study at the University of Pittsburgh (Gornick, 2011 ), a sample of 18 distinct life-like mannequin heads were imaged with both the 3dMD system as well as a competing stereophotogrammetry system. A standard set of facial surface landmarks were then collected from each 3D image. Facial surface landmarks were also capture on each head using an engineering-grade mechanical arm 3D digitizer. A series of 378 linear distance measurements were then compared across all three methods using several different error magnitude statistics. Sub-millimeter error levels were observed for all 378 measurements when the 3dMD system was compared to either of the other two methods, suggesting very high levels of accuracy. Those interested in learning more about the technical validation of the 3dMD system, should see the following articles : Aldridge et al. 2005 ; Losken et al. 2005; Weinberg et al. 2006 ; Wong et al . 2008 ; Heike et al. 2009 .
3D Facial Imaging Protocol
Prior to 3D image capture, care was taken to clear away any scalp hair obscuring the subject's face . This was accomplished through a variety of means including the application of hairnets, hair bands and various types of pins and clips. In addition, each subject had a handful of facial landmarks (pronasale , gnathion, left/right tragion) marked directly on the skin with a liquid eyeliner pencil, in order to facilitate the subsequent identification of the these points on the resulting 3D facial model.
The subject was seated directly in front of the camera system and positioned so that their head was centered between the imaging pods. The subject's head was positioned slightly upward (about 15-degrees off Frankfort horizontal) in order to ensure adequate coverage of the subnasal region. The subject was then instructed by the camera operator to keep their face still, with a relaxed and neutral facial expression, keeping their eyes open and pupils directed slightly upward (to emphasize the white of the eye and make the commissures more conspicuous). For young children is was sometimes necessary to have them sit on a parents lap during the image capture process.
Once the image was taken, the 3D model was processed (approximately 30 seconds) and visualized to evaluate quality. The camera operators were trained to inspect the 3D models for motion artifacts, mesh defects, camera calibration errors, missing surface data, and non-neutral facial expressions. Additional 3D captures were taken until one of sufficient quality was obtained.
Post-Capture Image Processing
Each 3D model (in .tsb format) was loaded into the 3dMDpatient software program. Extraneous data were then removed from each surface model, including most of the subject's neck and shoulders. The cleaned 3D model was then oriented to achieve clear frontal view of the face and re-saved, preserving the new orientation. No hold-filling, mesh-repair or smoothing routines were applied to any of the surfaces.
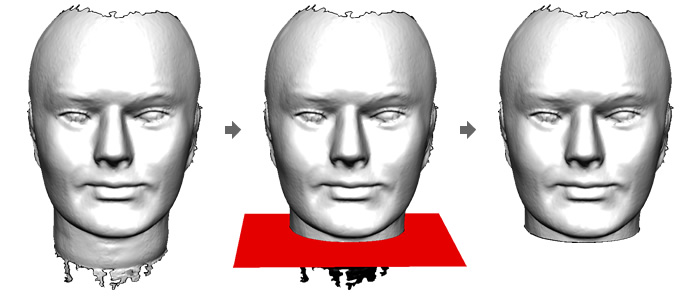
Finally, each cleaned 3D surface was exported as an Object Wavefront (.obj) file.
Landmarking of 3D Facial Surfaces
The Landmarking Process
Each cleaned and re-oriented 3D facial model was loaded into the 3dMDvultus software program, and using a custom template, a series of 24 facial landmarks were located manually on each surface (see list below). The landmarks were selected in a specific and strict order, with midline points collected first followed by bilateral points, moving in a superior to inferior direction. Any missing landmarks - typically due to a lack of adequate surface coverage or interference by scalp hair - were simply skipped . All landmarking was performed on 3D models with color and texture mapping active.
After the order and placement of the landmarks were double-checked for accuracy, each 3D model was saved again along with the associated landmarks. The x,y,z coordinate positions for all 24 landmarks were then saved to a simple text file.
All landmarking was completed at the University of Pittsburgh by a limited set of highly trained personnel (see training below).
3D Surface Landmarks and Definitions
The 24 facial surface landmarks included in the 3D Facial Norms Database are listed below, along with their definitions and description of the method used to identify them on the 3D facial surface. All of the included landmarks are derived from the traditional anthropometric canon. However, there are some inescapable and fundamental differences between traditional anthropometry and 3D surface anthropometry that must be considered. Most importantly, in traditional anthropometry, several facial landmarks (e.g., nasion) are identified through direct palpation of the soft tissues. Since there is no equivalent procedure in 3D surface anthropometry for identifying such points, one must rely solely on visual cues .
This fact imposes limitations on the number and kinds of landmarks that can be located reliably on a 3D facial surface. Some common landmarks, such as gonion, simply cannot be localized on a 3D facial surface with any consistency, because good visual cues are lacking. Compared to a skull, the human face has remarkably few anatomically relevant and useful landmarks. For a landmark to be both anatomically relevant and useful, it should ideally: (1) be related to some important or fundamental aspect of the morphological feature being described ;(2) be anatomically homologous across all subjects in the sample ;(3) be defined and identified in a manner that is not solely contingent on the location of other landmarks ; and (4) be capable of reliable identification by human observers.
The 24 landmarks included here were carefully chosen based on the criteria outlined above, with the additional consideration of maximizing coverage of the facial surface while, at the same time, minimizing the presence of redundant points.
The landmarks listed below are presented in the order collected:
NASION
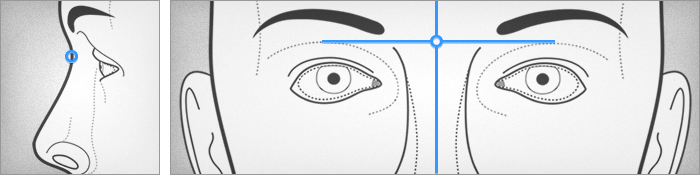
Nasion (n) can be a challenging landmark to identify reliably using 3D surface anthropometry. Soft tissue nasion is defined as the point immediately overlying the nasofrontal suture in the midline. In traditional direct anthropometry, nasion is typically identified through palpation. On 3D facial surfaces, alternative methods must be used. The landmark should be placed in the midline between the orbits, vertically at the level of the uppermost sulci created by the eyelids. To facilitate identification , the operator can imagine a line connecting the right and left superior palpebral sulci. Nasion is often mistaken for sellion, which is defined as the deepest midline point of the angle formed between the nose and forehead. When the face is viewed in profile, nasion should be slightly superior and anterior to sellion. In individuals with very shallow nasofrontal angles, however, the two points can approximate each other.
PRONASALE
Pronasale (prn) is defined as the most protrusive point on the nasal tip in the midline. Care must be taken when locating pronasale because it can be influenced by orientation. The point is easiest to place on the 3D facial model in the frontal view, but its position must be verified in the lateral (profile) view.
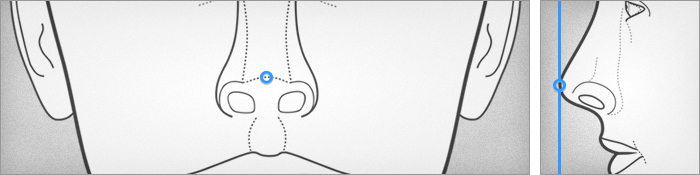
SUBNASALE
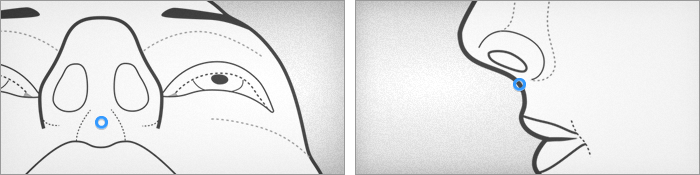
Subnasale (sn) is located at the apex of the nasolabial angle in the midline, where the inferior border of the nasal septum meets the skin of the upper lip. After placing the point on the 3D facial model , the position of subnasale must be verified with face in lateral (profile) view. Subnasale can sometimes be difficult to locate when the nasolabial angle takes the form of a sloping curve. In these cases , it is typical to place the point at the most concave position along the curve.
LABIALE SUPERIUS
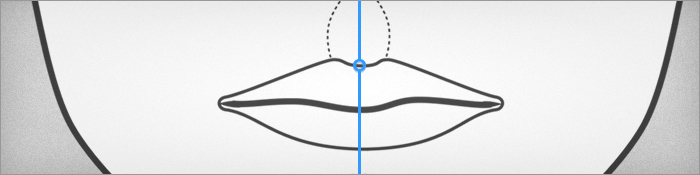
Labiale superius (ls) is located in the midline - between the philtral ridges - along the vermillion border of the upper lip. The point is typically identified on the 3D facial model in frontal view. Labiale superius is highly susceptible to distortion due to non-neutral facial expressions; care must be taken to inspect the 3D model prior to landmarking.
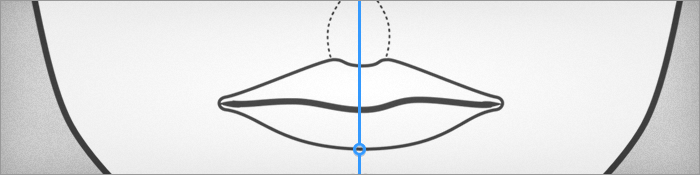
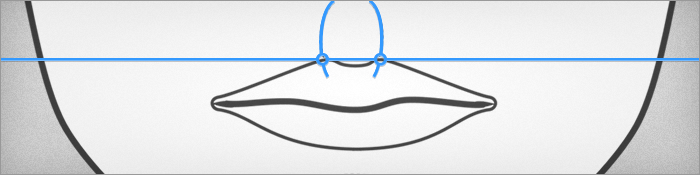
STOMION
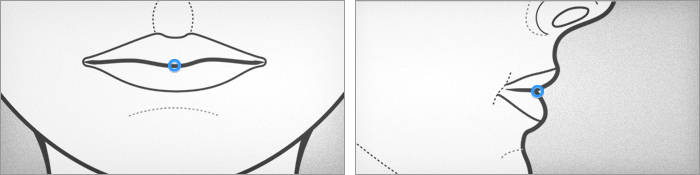
Stomion (sto) is located along the labial fissure in the midline. When the lips are closed, locating stomion is relatively straightforward. The point can still be identified when the lips are apart by placing the landmark along the inferior free margin of the upper lip. According to Kolar and Salter (1997), in cases where the lips exhibit significant asymmetry, “…stomion will not be precisely in the midline, but can be located below the philtrum.” The point is typically identified on the 3D facial model in frontal view.
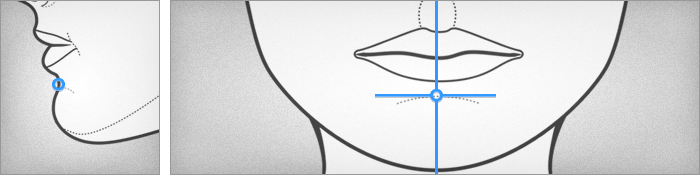
LABIALE INFERIUS
Labiale inferius (li) is located in the midline along the inferior vermillion border of the lower lip. The point is typically identified on the 3D facial model in frontal view. Since labiale inferius is located below the labial fissure, caution must be taken when the 3D model exhibits an open-mouth posture. Depending on the degree of mouth openness, the landmark may be invalid and should not be collected . Labiale superius is also highly susceptible to distortion due to non-neutral facial expressions; care must be taken to inspect the 3D model prior to landmarking.
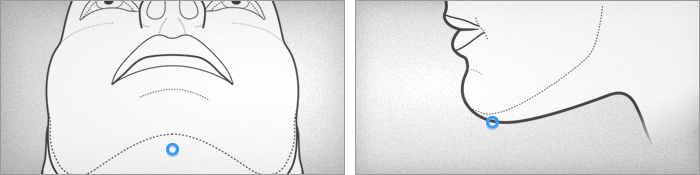
SUBLABIALE
Sublabiale (sl) is located at the midpoint of the labiomental groove or sulcus. As such, sublabiale demarcates the inferior extent of the cutaneous lower lip. The landmark is typically identified on the 3D facial model in frontal view, but its placement should be verified with the face in lateral (profile) view. In situations where the mandible deviates to one side or the other, sublabiale may not be in the same exact midline plane as defined by points on the upper portions of the face. Since sublabiale is located below the labial fissure, caution must be taken when the 3D model exhibits an open-mouth posture. Depending on the degree of mouth openness, the landmark may be invalid and should not be collected .
GNATHION
Gnathion (gn) is a midline point located on the inferior surface of the chin (mandible). It is located immediately adjacent to the corresponding boney landmark on the underlying mandible. Correct placement of the gnathion on the 3D facial model can only be effectively determined with the face in lateral (profile) view. Gnathion should be placed along the contour of the chin, just at the point where it turns to the underside. The most common mistake is placement of the landmark either too far anterior or too far posterior. In situations where the mandible deviates to one side or the other, gnathion may not be in the same exact midline plane as defined by points on the upper portions of the face. Like other landmarks located below the labial fissure, caution must be taken when the 3D model exhibits an open-mouth posture. Depending on the degree of mouth openness, the landmark may be invalid and should not be collected.
ENDOCANTHION (Right and Left)
Endocanthion (en) is a bilateral landmark located at the medial corner of the eye where the upper and lower eyelids meet. The landmark is sometimes mistakenly identified as the medial termination point of the white portion of the eye; the true endocanthion is located more medially. Endocanthion is fairly straightforward to locate on 3D facial models, and can be reliably identified with the eyes in an open or closed state. The presence of epicanthal folds, however, can interfere with the identification of endocanthion. In this situation, Kolar and Salter (1997) recommend using the point where the fold crosses the eye fissure.
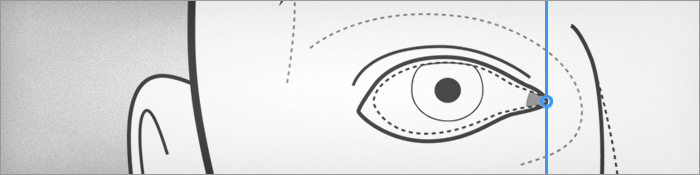
EXOCANTHION (Right and Left)
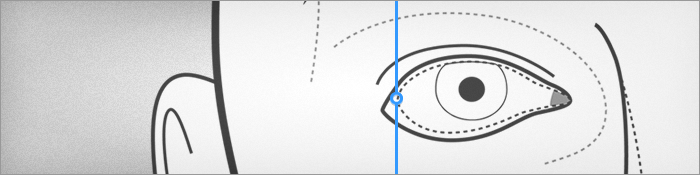
Exocanthion (ex) is a bilateral point located at the lateral corner of the eye where the upper and lower eyelids meet. It is effectively the lateral termination point of the white portion of the eye . Exocanthion can by challenging to identify on 3D facial models. Unlike endocanthion, exocanthion cannot be reliably identified if the subject's eyes are closed. Even partial eye closure can significantly obscure its location. Other hindering factors can include advanced age (as the skin folds begin to droop) and the presence of excessive eye makeup or eyelash enhancements. Exocanthion is also highly susceptible to distortion due to non-neutral facial expressions; care must be taken to inspect the 3D model prior to landmarking. Due to all of these factors, exocanthion may be difficult or impossible to landmark. Having the subject fully open their eyes and direct their pupils upward during 3D image capture can greatly improve the ability identify this landmark.
ALARE (Right and Left)
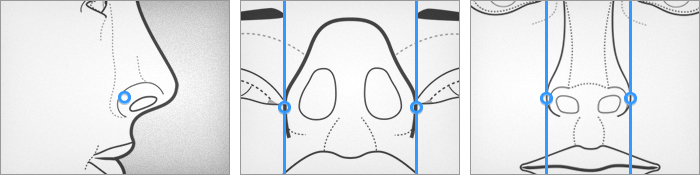
Alare (al) is a bilateral point defined as the lateral-most projection of the nasal ala. Alare is probably the most difficult and time-consuming landmark to reliably identify on 3D facial models. Because the ala has a 3D convex shape, finding the lateral-most point (local maxima) requires a fair amount of trial and error with placement. Typically, the landmark must be initially placed on the 3D model through estimation. Its placement on the ala must then be verified in the anterior-posterior direction (by inspecting the model in subnasal view) and the superior-inferior direction by inspecting the model in frontal view) and adjusted in an iterative process. Due to the ala's propensity to flare out with certain facial expressions, extra care must be taken to inspect the 3D model prior to landmarking.
ALAR CURVATURE POINT (Right and Left)
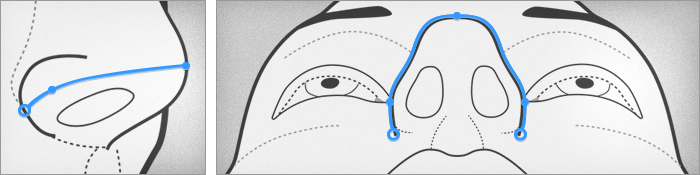
The alar curvature point (ac) is a bilateral landmark located along the crescent-shaped crease or fold formed where the alar cartilage meets the skin of the cheek. Traditional anthropometric descriptions locate this landmark at the most posterolateral position along the crease (Kolar and Salter, 1997). However, without a standard head orientation, we have found that the alar curvature point is difficult to reliably identify on 3D facial surface models. An alternative approach to locating the alar curvature point is to imagine a line connecting pronasale (on the nasal tip) with the superior-most extent of the alar crease. Then sweep along the crease in a superior to inferior direction until the longest linear distance is achieved and place the landmark at this level. On infants, the alar curvature point and alare may be located very close to one another and difficult to distinguish. The alar curvature point is highly susceptible to distortion due to non-neutral facial expressions; care must be taken to inspect the 3D model prior to landmarking.
SUBALARE (Right and Left)
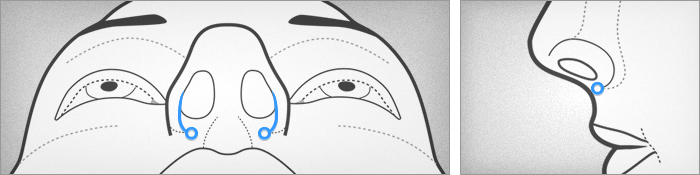
Subalare (sbal) is a bilateral landmark located below the nostril opening at the point where the infero-medial continuation of the alar cartilage inserts into the skin of the upper lip. Subalare is located at the lower bound of this insertion. In some individuals, there is no clear insertion point because the ala is continuous with the base of the columella, forming a slight ridge along the entire inferior margin of the nostril. In these cases, the most inferior point along the ridge can be substituted for subalare . Typically, subalare is easiest to identify with the 3D model in frontal view or tilted slightly upward to reveal the subnasal region. Subalare is highly susceptible to distortion due to non-neutral facial expressions; care must be taken to inspect the 3D model prior to landmarking.
CRISTA PHILTRI (Right and Left)
Christa philtri (cph) is a bilateral landmark located where the philtral ridges or crests meet the vermillion border of the upper lip. It is easiest to identify with the 3D facial model in frontal view or tilted slightly upward to reveal the contours of the upper lip. This landmark can be difficult to visualize in individuals with a poorly defined philtrum. In individuals with clefts of the lip, surgical reconstruction often obscures the landmark. The presence of excessive lipstick and lip liners can also be problematic. Christa philtri is highly susceptible to distortion due to non-neutral facial expressions ; care must be taken to inspect the 3D model prior to landmarking.
CHELION (Right and Left)
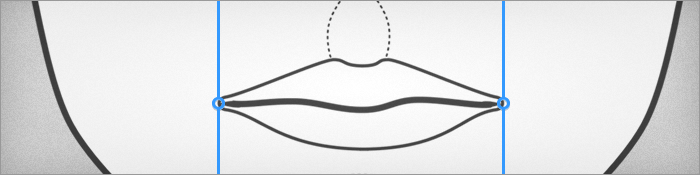
Chelion (ch) is a bilateral landmark located at the outermost corner (commissure) of the mouth where the upper and lower lips meet. As such, it demarcates the lateral extent of the labial fissure. The landmark is typically placed with the 3D facial model in standard frontal view. In individuals of advanced age, chelion may be difficult to locate due to a loss of structural integrity in the skin at the edge of the mouth. Chelion is highly susceptible to distortion due to non-neutral facial expressions; care must be taken to inspect the 3D model prior to landmarking.
TRAGION (Right and Left)
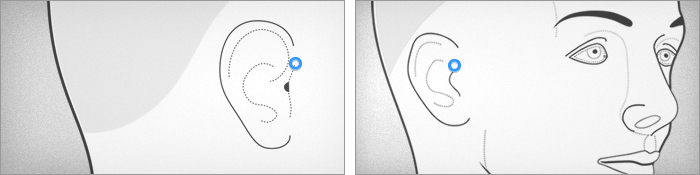
Tragion (t) is a bilateral landmark located within the small notch at the superior extent of the tragus (cartilaginous projection just anterior to the auditory meatus), where the cartilage meets the face . The landmark must be placed with the 3D facial model in lateral (profile) view. The presence of even small amounts of hair from the scalp or sideburns can obscure tragion on the 3D model. This is why management of the subject's hair prior to image capture is essential, even though at times the problem is unavoidable. Tragion can sometimes be difficult to visualize on 3D facial models even when the anatomy is not obscured. With certain 3D system configurations, for example, distortion of the ears can occur due to the camera's limited field of view. For this reason, we always recommend pre-marking tragion directly on the subject's face with a water-based skin pen prior to imaging.
Landmark Collection Training
Individuals responsible for landmarking 3D facial surfaces undergo a two-phase training regimen. In the first phase, the uninitiated trainee is instructed to landmark a standard training set of 10 3D facial models with all 24 landmarks. The landmark placement on each 3D model is then reviewed by the PI (Weinberg) and feedback is provided through a one-on-one instruction session. Armed with this feedback, the trainee then begins the second phase. Here they collect the same 24 points twice on a second independent training set of 20 3D facial models, in order to allow for the quantification of the intraobserver error associated with their landmark localization. They are instructed to allow a minimum of 48 hours to pass between the first and second landmarking sessions to minimize recall bias . Once they have completed the landmarking, the associated 3D coordinates are error checked for gross errors (e.g., right-left reversals) and compared across the two sessions. Intraclass correlation coefficients are calculated for each landmark, separately for each of the three principal coordinate axes (x,y,z ). This approach makes it possible to identify any deficiencies in landmark placement in a highly detailed manner, allowing for targeted remediation. Every coefficient must be 0.90 or greater for a trainee to proceed with landmark collection on real data. Additional instruction is provided for trainees who fail any portion of the second phase of training. They may proceed only once they have adequately addressed the deficiency.
In order to keep landmarking personnel on track, biweekly group meetings are held with the PI (Weinberg ) to review any difficult or confusing cases. These meetings are designed to be informal and educational in nature and are attended by a number of staff and students who are engaged in similar facial landmarking projects. All meeting participants are encouraged keep a running list of any difficulties or uncertainties they encounter during landmarking. Typically, the 3D facial model in question will be called up and the landmark placement openly discussed among the group until the issue is resolved. If corrective action is required, the landmarker is instructed to make the necessary changes and re-save the data . By reviewing everyone's work periodically in this manner, the landmarkers eventually learn how to avoid common problems and make correct judgments in uncertain situations.
Inter-Landmark Distances Derived from 3D Facial Surfaces
A pre-defined set of 29 linear distances was calculated from each subject's 3D facial landmark coordinates through simple Euclidean geometry. These distances correspond to traditional facial anthropometric measurements as defined by Farkas and others, and were chosen for their clinical relevance and because they comprise a core set of variables for describing general facial form. Of course users are capable of generating any number of alternative inter-landmark distances directly from the raw coordinate data available through the 3D Facial Norms Database.
- Cranial base width
- Upper facial depth (Right)
- Upper facial depth (Left)
- Middle facial depth (Right)
- Middle facial depth (Left)
- Lower facial depth (Right)
- Lower facial depth (Left)
- Morphological facial height
- Upper facial height
- Lower facial height
- Intercanthal width
- Outercanthal width
- Palpebral fissure length (Right)
- Palpebral fissure length (Left)
- Nasal width
- Subnasal width
- Nasal protrusion
- Nasal ala length (Right)
- Nasal ala length (Left)
- Nasal Height
- Nasal Bridge Length
- Labial fissure width
- Philtrum width
- Philtrum length
- Upper lip height
- Lower lip height
- Upper vermilion height
- Lower vermilion height
- Cutaneous lower lip height
Because these 29 measurements are all derived from 3D facial surfaces, caution should be taken before comparing or combining these measurements with those collected using traditional direct anthropometry (i.e., with calipers, rulers and cloth tape). In addition to subtle differences in landmark identification between these two methods, many measurements obtained through direct anthropometry require some degree of deformation - however slight - of the pliable soft tissues of the face with the caliper tips. Obviously , measurements computed from 3D surface models do not involve such deformation. One must be cognizant of these method differences to avoid potential data stratification effects, which could lead to spurious findings.
All measurements are in millimeters.
Availability of 3D Facial Surfaces
The original 3D facial surface files for each individual in the study are available to users through the 3D Facial Norms Database. The surface files are provided in object wavefront (.obj) format, without the associated color/texture mapping files. This means that users will be able to display the underlying geometry, but not the surface color and texture associated with subjects' faces. Most 3D visualization programs - including free programs like MeshLab - are able to open and manipulate files in .obj format . To gain access to these files, the user must specify their intent on the Data Access Request form and must have the appropriate IRB designation. The user should carefully review the Data Use Certification (DUC) document to ensure that they understand the ways that FaceBase human data may and may not be used.
Additional Anthropometric Measurements
A handful of additional linear distance measurements obtained through traditional direct anthropometry are also available through the 3D Facial Norms Database. These are generally large measurements of the head and face, which are either difficult or impossible to capture through indirect 3D surface anthropometry .
- Maximum cranial width
- Minimum frontal width
- Maximum facial width
- Mandibular width
- Maximum cranial length
Trained personnel at each recruitment site obtained these measurements with spreading calipers, in accordance with the methods described in Kolar and Salter (1997).
All measurements are presented in millimeters.
DNA Collection Protocol
Oragene collection kits (DNA Genotek) were used to obtain saliva samples on all study participants . Adults and children six years and older provided a single kit. Children under the age of six were asked to provide two kits each to account for the low yield that sometimes occurs with these individuals . Cheek swaps were used for children too young to provide adequate spit samples. Sugar packets were available for participants who had difficulty producing enough saliva. All kits were sent to the University of Pittsburgh for extraction.
Genotyping
In collaboration with the Center for Inherited Disease Research (CIDR), 3D Facial Norms participants have been genotyped using a genome-wide association (GWA) array consisting of 964,193 SNPs (Illumina OmniExpress+Exome v1.2) plus an additional 4322 custom SNPs chosen based on prior craniofacial genetic studies.
The genomic data is available to researchers through dbGaP’s controlled access repository:
Accession number: phs000949.v1.p1
Data Cleaning Procedures
Prior to uploading data into the 3D Facial Norms Database, several data cleaning actions were performed .
3D Facial Landmark Coordinates
The identification of misplaced landmarks (e.g., order errors or right/left reversals) is accomplished by importing each individual's set of x,y,x coordinates into a custom program designed to visually inspect the relative spatial arrangement of landmarks. Each individual's 3D landmarks are projected onto a two dimensional plane and connected with a series of predefined lines creating a wireframe model. The wireframe is designed such that a correctly landmarked face will have no overlapping lines. Inverted or misplaced landmarks are revealed visually when the normal arrangement of line segments is distorted by overlapping lines or abnormal arrangements.
Additional logic rules are defined that highlight erroneously placed landmarks based on a coordinate component relative to another landmark in the configuration. For example, if midline landmark points are placed on a face in the incorrect order, their relative Y-axis positions can reveal the erroneous landmark. Or consider the inversion of left and right points, the relative X-axis positions will reveal the errors, since the X-value of the left point should always be greater than the right.
After a landmarking error is discovered, the 3D facial model is re-landmarked and the updated coordinates are re-saved. Another program was developed to automatically collect and assemble every subject's coordinates into a centrally located database. Every time this program is run, it automatically updates the local database with the most recent landmark information.
3D Linear Distance and Caliper Measurements
To expose potentially erroneous measurements and outliers, Z-scores were calculated for each measurement variable for each individual in the dataset. These scores were calculated relative to other individuals in the dataset with the same sex, ancestry and age. For individuals under 20 years old, measurements were compared within their whole number age group. For individuals 20 years old and older, measurements were compared with individuals +/- 2 years. A filter is applied to select and highlight any measurements with an absolute value Z-score greater than 3. If the measurement was obtained through traditional direct anthropometry, the value was confirmed on the original collection form taken at the time of measurement . If the measurement was derived from 3D landmarks, the landmark positions were verified through visual inspection of the 3D surface model. Any and all incorrect values were fixed and logged.
Demographic Data
Outlier detection routines were run to identify any potentially erroneous data points. If a problematic value is detected, the data is then verified by cross-checking the original source documents. Any and all incorrect values were fixed and logged.
Variable Naming Conventions and Coding
Unique Subject Identifiers
Each subject in the 3D Facial Norms Database is provided with a unique random 10-digit numeric identifier .
Demographics
- Sex: 1 = Male; 2 = Female
- Age (years)
- Height (cm)
- Weight (kg)
- Hispanic: 0 = No; 1 = Yes
- Ancestry: 1 = European Caucasian
3D Landmark Coordinates
| Landmark id | 3D Facial Norms Variable id |
|---|---|
| Nasion | n_x; n_y; n_z |
| Pronasale | prn_x; prn_y; prn_z |
| Subnasale | sn_x; sn_y; sn_z |
| Labiale Superius | ls_x; ls_y; ls_z |
| Stomion | sto_x; sto_y; sto_z |
| Labiale Inferius | li_x; li_y; li_z |
| Sublabiale | sl_x; sl_y; sl_z |
| Gnathion | gn_x; gn_y; gn_z |
| Endocanthion (Right): | en_r_x; en_r_y; en_r_z |
| Endocanthion (Left) | en_l_x; en_l_y; en_l_z |
| Exocanthion (Right) | ex_r_x; ex_r_y; ex_r_z |
| Exocanthion (Left) | ex_l_x; ex_l_y; ex_l_z |
| Alare (Right) | al_r_x; al_r_y; al_r_z |
| Alare (Left) | al_l_x; al_l_y; al_l_z |
| Alar Curvature Point (Right) | ac_r_x; ac_r_y; ac_r_z |
| Alar Curvature Point (Left) | ac_l_x; ac_l_y; ac_l_z |
| Subalare (Right) | sbal_r_x; sbal_r_y; sbal_r_z |
| Subalare (Left) | sbal_l_x; sbal_l_y; sbal_l_z |
| Crista Philtri (Right) | cph_r_x; cph_r_y; cph_r_z |
| Crista Philtri (Left) | cph_l_x; cph_l_y; cph_l_z |
| Chelion (Right) | ch_r_x; ch_r_y; ch_r_z |
| Chelion (Left) | ch_l_x; ch_l_y; ch_l_z |
| Tragion (Right) | t_r_x; t_r_y; t_r_z |
| Tragion (Left) | t_l_x; t_l_y; t_l_z |
3D Inter-Landmark Distances
| Measurement id | 3D Facial Norms Variable id |
|---|---|
| Cranial Base Width | CranBaseWidth |
| Upper Facial Depth (Right) | UpFaceDepth_R |
| Upper Facial Depth (Left) | UpFaceDepth_L |
| Middle Facial Depth (Right) | MidFaceDepth_R |
| Middle Facial Depth (Left) | MidFaceDepth_L |
| Lower Facial Depth (Right) | LowFaceDepth_R |
| Lower Facial Depth (Left) | LowFaceDepth_L |
| Morphological Facial Height | MorphFaceHeight |
| Upper Facial Height | UpFaceHeight |
| Lower Facial Height | LowFaceHeight |
| Intercanthal Width | InCanthWidth |
| Outercanthal Width | OutCanthWidth |
| Palpebral Fissure Length (Right) | PalpFisLength_R |
| Palpebral Fissure Length (Left) | PalpFisLength_L |
| Nasal Width | NasalWidth |
| Subnasal Width | SubNasalWidth |
| Nasal Protrusion | NasalPro |
| Nasal Ala Length (Right) | NasalAlaLength_R |
| Nasal Ala Length (Left) | NasalAlaLength_L |
| Nasal Height | NasalHeight |
| Nasal Bridge Length | NasalBdgLength |
| Labial Fissure Width | LabFisWidth |
| Philtrum Width | PhilWidth |
| Philtrum Length | PhilLength |
| Upper Lip Height | UpLipHeight |
| Lower Lip Height | LowLipHeight |
| Upper Vermilion Height | UpVermHeight |
| Lower Vermilion Height | LowVermHeight |
| Cutaneous Lower Lip Height | CutLowLipHeight |
Caliper-Based Anthropometric Measurements
| Measurement id | 3D Facial Norms Variable id |
|---|---|
| Maximum Cranial Width | MaxCranWidth |
| Minimum Frontal Width | MinFrntWidth |
| Maximum Facial Width | MaxFaceWidth |
| Mandibular Width | MandWidth |
| Maximum Cranial Length | MaxCranLength |
3D Facial Surface Models
The .obj file for each subject is idd with their unique 10-digit numeric identifier.
Genotypes
Coming soon...
Structure of Data Output Files
Users with the proper permissions are able to download individual-level data elements. Demographic data, 3D landmark coordinates and all measurements are provided as comma separated values (.csv) files , which can be opened in any spreadsheet program. The variable ids at the top of each column conform to the scheme described above.
Using the Z-Score Tool
Z-scores are commonly used by clinicians to assess where a given individual sits in relation to the general population on some measured aspect of the phenotype. When population-based normative data is available, one is able to determine how many standard deviations an individual is from others of the same age, sex and ancestry. In the craniofacial context, Z-scores can be useful for pre-surgical planning , post-surgical outcome assessment, syndrome delineation, and in some cases, genetic counseling. Now that 3D stereophotogrammetry is becoming quite common in clinical settings, it is essential to be able to produce Z-scores based on measurements obtained with the same technology.
The simple interactive Z-score tool provided through the 3D Facial Norms Database allows a user to automatically generate Z-scores based on 3D surface measurements. First the user selects the sex, age and ancestry of the individual they are seeking to compare. Then the user selects the measurement of interest. Finally, the user enters the individual's measurement value. The resulting Z-score indicates in standard deviations how this individual compares to his/her peers. The process can then be repeated for additional measurements and/or individuals.
Like any comparison of this nature, it is essential that the measurement be taken correctly on the individual to be compared in order for the results to be accurate. It is also critical that equivalent methods be used (3D surface anthropometry or traditional direct anthropometry) when conducting such a comparison. Please see the preceding sections describing which methods were used to collect which measurement variables.
Citing the 3D Facial Norms Database in Reports and Presentations
Use of these data and summary statistics is subject to the conditions laid out in the FaceBase Data Use Certification.
Please refer to the FaceBase guidelines on citing our work. We are funded by NIDCR grant 1-U01-DE020078.
Future Plans for Repository Expansion
Immediate plans for the future include expanding both the age range and ethnic categories contained within the normative database. The 3D Facial Norms database was designed from the outset to be flexible , so that it can be easily scaled to accomplish these goals.
Contributing to the Database
For this resource to reach its full potential, we will need as much high-quality data as possible . If you are an investigator interested in contributing data to this resource, please contact the Principal Investigator, Seth M. Weinberg, PhD.
Acknowledgments
University of Pittsburgh
- Seth M. Weinberg, PhD, Principal Investigator
- Mary L. Marazita, PhD, Co-Principal Investigator
- Pooja M. Gandhi, MS, Study Coordinator
- Zach D. Raffensperger, BS, Principal Programmer and Web-Developer
- Rebecca S. DeSensi, BS, Database Manager
Seattle Children's Research Institute
- Carrie L. Heike, MD, Co-Investigator
- Michael L. Cunningham, MD, PhD, Co-Investigator
- Laura Stueckle, MPH, Study Coordinator
- Linda Peters, BA, Research Associate
- Erik Stuhaug, AAS, Medical Photographer
- Eden Palmer, BS, Medical Photographer
- Trylla Tuttle, BA, Research Assistant
University of Texas Health Science Center (Houston)
- Jacqueline T. Hecht, PhD, Co-Investigator
- Chung How Kau, BDS, PhD, Consultant (currently at UA Birmingham)
- Lidia Leonard, BS, Clinical Research Coordinator
- Maria Elena Serna, BS, Database Specialist
- Rosa N. Martinez, Clinical Research Coordinator
Funding
The project is funded by the following grants from the NIDCR: 1-U01-DE020078
Disclaimer
The PIs or Co-Is on this project have no financial disclosures or conflicts of interest to report .